
Patients with teary eyes often feel as if they are constantly crying
Do you have teary eyes? Have you learned to live with constant watering, or been told that there is no treatment? Epiphora, the medical term for excessive tearing, is a common complaint the cause of which can be difficult to isolate. Patients often suffer from this condition silently for years, or become accustomed to its presence after failing to find the source. Excessive tearing can interfere with many activities in daily living. Patients may experience difficulty with reading and driving due to blurriness and build-up of eye secretions. There is also the added annoyance of having to carry tissues to dry the eyes, and frequent tissue use can cause skin irritations.
To better understand tearing problems and isolate the source, it is first important to know where tears come from and how they function. A healthy tear film is a vital aspect of ocular health. Tears provide key nutrients to the eye and contain immunoglobulins (antibodies) which help to combat infection. They also remove foreign bodies, debris and infectious agents.
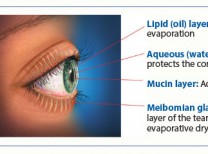
Tears are produced in the lacrimal gland and are comprised of three layers (the outermost fatty layer, the middle aqueous layer, and the innermost mucus layer). This gland is located in the deeper tissues of the upper outer eyelid. Once formed, tears exit the gland openings of the upper eyelid, bathe the surface of the eye and then migrate across the ocular surface. Eyelid blinking mechanically determines the directionality of tear flow. As the eyelids blink, the tears are directed towards the inner eyelids. Once in this region, tears enter the lacrimal drainage system through the puncta (small openings in the inner corner of the upper and lower eyelids). After flowing down through the lacrimal sac (tear sac), tears drain out through the nose.
Excessive tearing may be congenital or acquired and have a variety of causes, including eyelid inflammation, eyelid malposition and malfunction of the lacrimal system itself. Eyelid inflammation may disrupt the formation of the outermost fatty layer of the tear film, leading to its instability and premature evaporation. This results in dry eye, irritation and reflexive tearing, as the body attempts to ameliorate the discomfort. Inflammation must be controlled to help restore proper lipid production.
Eyelid malposition can cause tearing as well. Different types of malposition exist. Entropion occurs when the eyelid margin is turned inwards. The eyelashes rub against the eye and cause irritation. This irritation causes secondary reflexive tearing. Ectropion occurs when the eyelid margin is turned outward and thus not in contact with the eye. The moist inner surface of the eyelid, which is normally not directly exposed to the environment, is now subject to air flow and direct contact. This irritation leads to tearing. Additionally, the punctum is not properly aligned to receive the tears. This is similar to having the drainage hole misaligned with the sink. In most cases, eyelid malposition can be repaired with a short outpatient procedure.
 Finally, the lacrimal system itself may be responsible for epiphora. Optimal tear performance requires proper tear production and flow. Occasionally, epiphora is caused by the production of excessive amounts of tears. This condition is less common, but may be amenable to treatment with Botox®. Tiny injections of botulinum toxin into the lacrimal gland can decrease tear output. In the vast majority of cases, a blockage of the drainage system is the culprit. In children, a membrane that is located at the end of the nasolacrimal duct, just before it exits into the nose, usually causes the blockage. An outpatient probing of the lacrimal system usually alleviates this blockage. In adults, the blockage is usually an acquired closure of the nasolacrimal duct itself. Once blocked, a detour must be created to bypass this area through a procedure called dacryocystorhinostomy (DCR). During a DCR, a small incision is made at the side of the nose at the level of the nasal bridge. A small amount of bone is removed from the side of the nose so that tears can flow out of the eye. A silicone stent is left in place for 3-6 months to maintain patency of the new pathway.
Finally, the lacrimal system itself may be responsible for epiphora. Optimal tear performance requires proper tear production and flow. Occasionally, epiphora is caused by the production of excessive amounts of tears. This condition is less common, but may be amenable to treatment with Botox®. Tiny injections of botulinum toxin into the lacrimal gland can decrease tear output. In the vast majority of cases, a blockage of the drainage system is the culprit. In children, a membrane that is located at the end of the nasolacrimal duct, just before it exits into the nose, usually causes the blockage. An outpatient probing of the lacrimal system usually alleviates this blockage. In adults, the blockage is usually an acquired closure of the nasolacrimal duct itself. Once blocked, a detour must be created to bypass this area through a procedure called dacryocystorhinostomy (DCR). During a DCR, a small incision is made at the side of the nose at the level of the nasal bridge. A small amount of bone is removed from the side of the nose so that tears can flow out of the eye. A silicone stent is left in place for 3-6 months to maintain patency of the new pathway.
In summary, proper treatment of excessive tearing requires identification of the source. There are many causes of tearing; sometimes more than one condition is contributing to the problem. Excessive tearing problems are often overlooked but can have a significant impact on a patient’s functioning. Many people have slowly adapted to its presence and changed their lifestyle accordingly. The good news is that tearing is treatable. The cause is sometimes difficult to isolate, but thorough investigation and subsequent treatment can greatly ameliorate your symptoms and allow you to put those tissues away!
Dr. Hui is an Oculoplastic surgeon fellowship trained to treat patients with Eyelid, Lacrimal and Orbital conditions. She has trained and been on faculty at the world renowned Bascom Palmer Eye Institute in Miami, FL (consistently ranked the #1 eye hospital in U.S. News and World Report). She has relocated to her native Southern California opening The Eyelid Institute in Palm Desert. 760.610.2677.













































Comments (3)
Hi,
Hope you are well.
I am writing to you regarding the eye image you are using on your website. I am currently working on a website for a non-profit organisation and am looking for a photo of a teary eye.
I would like to kindly ask if it would be possible to use your photo.
The charity is based in Ireland.
Blessings,
Karolina
Thank you, Karolina.
The photo is from 4 years ago and it would take time to find the source, however many similar photos can be purchased for $1 from sites like Adobe Stock and others. This one may have come from https://www.dollarphotoclub.com.
All the best with your venture ~
Lauren
“Aloha” Dr Del Sarto – I’ve been battling with ‘dry eye’ for a couple of years now, and have still not found any effective treatment. I’d never had a problem until I had a cold. The cold got better, but my right eye still watered. I thought I must have had some kind of residual infection. Antibiotics did not help. I was told the duct was blocked. It was irrigated several times. The duct seemed to be open ‘sometimes’ but then the tearing would resume. The diagnosis seemed to change according to what day of the week it was. One doctor first told me it was probably an allergy, and gave me antihistamine drops. Then more irrigation. Then ‘reflexive tearing’ (despite the fact that tearing was only in one eye). Then a punctal plug – no relief. Then the lacrimal duct surgery done earlier this year (I took a while to screw up my courage for that one). But again, no relief. The ONLY time my eye was completely normal for 9 days was when I was on steroid drops which were like a miracle for 9 days, but on Day 10 the tearing resumed and the drops became ineffective. I’m at my wit’s end. I’ve seen FIVE ophthalmologists and now my Kaiser docs are telling me they won’t refer me to an outside source unless I have a ‘second opinion’. You can imagine that by this time, I’m rather frustrated. I read about the Bascom Palmer clinic as being the # 1 rated in the country, and I was delighted to see that you had worked there and relocated to Southern California! I am spending time in Santa Barbara for the next few months and wondered if it would be possible to make an appointment to see you?
Sincerely,
Sharyn