Dry eye is a common condition that is often under-treated or under-addressed, especially here in the desert. Our local climate has many unique factors that contribute to “corneal surface disease” which is the new descriptive name for dry eye. Factors include low humidity, wind, particulate matter in the air, dust, pollens, lots of places with air conditioning, and our self-induced problems such as overseeding and planting a large variety of flowering plants and trees.
That said, there are a host of diagnostic tools available to the practitioner to help identify corneal surface disease and initiate treatment, including the following:
Questionnaires. If we don’t ask, you won’t tell us. Do your eyes ever feel dry or uncomfortable? Are you bothered by changes in your vision throughout the day? Do you ever use, or feel the need to use, eye drops?
Corneal topography. When the corneal surface is dry, it creates an irregular surface that can be identified when mapped and improved with treatment.
Lipid layer analysis. Studies show the majority of corneal dryness has an underlying evaporative basis (low oil) versus insufficient aqueous production.
Blink analysis. Our blink is so automatic that most times we are unaware of it. With automation, we can measure how often you blink and whether it’s a full or partial blink. Patients often have a history of facial or eyelid surgery from 10-15 years prior that can now interfere with proper blinking.
Tear osmolarity. As the moisture component of our tears evaporates, the osmolarity rises. High osmolarity has a strong correlation to corneal surface disease.
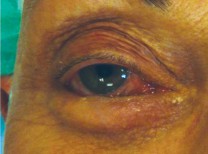
Red eye scaling. No one wants to have red eyes. We now have technology that allows us to objectively quantify how red the eyes actually are.
Matrix-mettaloproteinase-9. MMP-9 is a proteolytic enzyme released by compromised corneal epithelial cells. It is part of the inflammatory component of dry eye, and a simple in-office test is available to measure this.
Lissamine green and sodium fluorescein. These dyes along with rose bengal help identify damaged epithelial cells. Newer studies have shown that surface disease can be present without staining, but it is still a valuable tool.
Meibography. The meibomian glands are the primary lipid secretory glands. In patients as young as early 20s, dysfunction of these glands can be identified. Sometimes gland dropout occurs before symptoms occur. When there is significant gland loss, then supplementation is needed to replace the normal lipid secreted by these glands.
In summary, the science of corneal surface disease has come a long way in the last 5-10 years. Doctors can now treat patients earlier, and earlier treatment means less long-term damage and better outcomes.
Dr. Evans is the founding owner of Evans Eye Care in Palm Desert and can be reached at (760) 674.8806 or online at www.evanseyecare.com.













































Comments (0)