This editorial is offered in response to a November 2019 Desert Sun article regarding Phillip Bretz, MD, of La Quinta. In the article, we learned that the California Medical Board placed Dr. Bretz on probation due to factors related to offering cryoablation or “tumor freezing” to women seeking an alternative to surgery for early stage breast cancer.
As a breast cancer surgeon, researcher and patient advocate, I feel it necessary to challenge the negative impressions that the aforementioned article creates regarding cryoablation and Dr. Bretz, as well as the significant number of women seeking alternatives to “traditional” surgical treatment.
Although cryoablation is new to most readers, the procedure has served a role in the management of various cancers for decades. I began performing breast cryoablation in 2003, initially as a treatment of benign breast tumors called fibroadenoma, and later beginning in 2009 for early stage breast cancer as part of a national clinical trial sponsored by the American College of Surgeons.
The American College of Surgeons trial found cryoablation to be 100 percent effective at killing invasive breast tumors that were 1 cm or smaller and 92 percent effective for tumors up to 2 cm. As a result of the lessons learned from that trial, two additional national trials were launched evaluating cryoablation as an alternative to surgery for early breast cancer. Currently, the early results of both trials are promising, and I am honored to serve as lead principal investigator for one of them, the FROST Trial.1
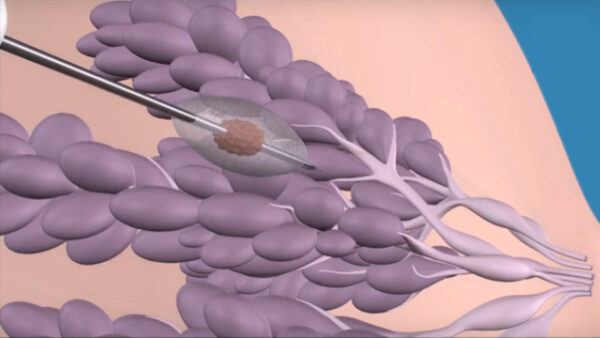
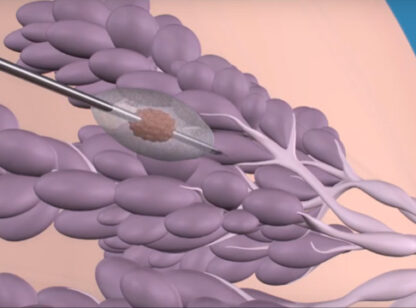
Internationally, the most promising breast cancer cryoablation experience comes from Japan where a respected surgeon has treated more than 300 women with estrogen-sensitive breast cancers 1.5 cm or smaller with cryoablation, radiotherapy and anti-estrogen therapy. This method has achieved a local control rate of 99 percent at 6 years average follow-up, and rivals what we can achieve with surgery. However, unlike surgery, cryoablation is a relatively pain-free procedure that can be performed through a 3 mm skin nick under local anesthesia as one-hour office procedure, with expedited return to normal activity and no long-term changes of breast shape or volume.
The primary issue raised in Dr. Bretz’s case was informed consent. Informed consent is essential for everything we do as cancer specialists, whether it’s lumpectomy, mastectomy, radiation, chemotherapy or other treatments. Each treatment can reduce cancer recurrence, but none is guaranteed to prevent recurrence. To varying degrees, each is also capable of causing physical or emotional harm that can impair short-term or long-term quality of life. The goal of informed consent is to ensure that patients are aware of these factors and possible alternatives so that they can determine which treatment regimen suits them best. As it turns out, compared to their doctors, patients tend to be more willing to accept risk and explore novel treatment options. However, as surgeon-innovators, we must also temper our enthusiasm to offer patients new treatment advancements by ensuring that they are fully informed about what is known, and more importantly, unknown about the innovations we offer.
Criticism of Dr. Bretz must also be judged in the context of a long history of surgeon-innovators and patient advocates who sought to make breast cancer surgery less disfiguring and less harmful to women. For example, if not for the advocacy and independent research efforts of Umberto Veronesi, an Italian surgeon, and Bernard Fisher, an American surgeon, women across the globe might still be subjected to radical mastectomy with removal of the entire breast, chest muscles and underarm lymph nodes. However, ultimate credit goes to the communities of women around the world who demanded different and better options for treating breast cancer. Today’s physicians are facing similar calls for better treatment options.
Cryoablation is not the only treatment for which Dr. Bretz challenged the status quo. Readers might also be surprised to learn that Dr. Bretz played a seminal, but similarly controversial, role in establishing tamoxifen as a treatment option for breast cancer. His early advocacy for tamoxifen stimulated national research efforts that ultimately established tamoxifen and similar medications as the preferred anti-cancer medication for women with estrogen-sensitive breast cancer. The human impact of this innovation is immeasurable.
It is safe to say that most physicians are motivated by their sworn professional obligation to “first do no harm” and by the desire to achieve the best possible outcome for their patients. However, it is no longer acceptable for physicians to be the sole judge of what is best for individual patients and to impose their own value-system on their patients. The new standard is “patient-centered care,” which the Institute of Medicine defines as “providing care that is respectful of, and responsive to, individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions.” This includes the decision to undergo cryoablation.
I am confident that the next 10 years will see cryoablation emerge as an established option for women with breast cancer. For this to happen, we must continue to monitor the outcome of ongoing trials and develop new trials for early, and later stage, breast cancer. Patients must understand that cryoablation is not intended to be a substitute for all other cancer therapies. Much like lumpectomy and mastectomy, cryoablation works best when supplemented by radiotherapy and/or drug therapy, as appropriate. Physicians must not hold cryoablation to a higher standard than we hold other cancer treatments. If a woman undergoes lumpectomy but later declines recommended radiation, we don’t insist that she return to the operating room for a mastectomy lest we fire her from our practice—at least most of us don’t. If a woman accepts tamoxifen but refuses chemotherapy despite its promise of additional survival benefit, we physicians still try to help her achieve the best possible outcome that can be achieved with tamoxifen alone.
At the end of the day, our highest responsibility is to equip patients with the knowledge required to make informed decisions about a range of imperfect treatment options. This practice will empower them to make healthcare decisions that best suit their physical and emotional needs from both a survival and quality of life perspective.
Dr. Holmes is a breast cancer surgeon and researcher in Los Angeles. For more information visit www.cryoablation.com or call (800) 203.5515.
Reference:
1) https://clinicaltrials.gov/ct2/show/NCT01992250









































Comments (2)
Dear Dr.Holmes I’m glad to contact with you
I am Dr\ Hamood from general surgery and I’m interested to make in practice under your guide about
Brest cancer cryosurgery
Hop that is possible and what is the procedures for that
thank you
Hello Dr. Hamood,
Thanks for your email. I’m a little unclear about your request. Please clarify what information you are looking for. Please feel free to email directly at drholmesmd50@gmail.com.
You can also read about cryoablation at http://www.cryoablation.com