Prostate cancer is the most common non-skin cancer in men. About 240,000 American men are diagnosed with prostate cancer each year, and in 130,000, the cancer is localized and low-risk. Although most prostate cancers are slow growing and unlikely to spread, most men receive immediate treatment with surgery or radiation. These therapeutic strategies are associated with short- and long-term complications, including impotence and urinary incontinence. Only a small number of men choose observational strategies, which may delay the initiation of curative therapy or avoid it completely.
Although the value of screening with a PSA (prostate-specific antigen) serum blood test has come under question recently, it is still the only widely available screening test for prostate cancer. While a single PSA value alone may have debatable value, PSA velocity (increase in PSA over time) and PSA density (PSA in ng/ml divided by prostate gland volume in cc’s) can be indicators of change, good or bad. Biopsy of the prostate gland is frequently necessary to distinguish between the causes of an elevated serum PSA.
Currently, the best test biomarker and indicator of prognosis for prostate cancer that we have is the Gleason score. The Gleason score is a number derived from the biopsy specimen a pathologist sees under a microscope. He or she looks for the most prominent cell type, the primary Gleason grade, then the second most prominent cell type, the secondary Gleason grade. The sum of the primary grade plus the secondary grade equals the Gleason score. The lowest Gleason grade is 1 and the highest is 5, so theoretically Gleason scores can range from 2 (1+1) to 10 (5+5). Years ago, doctors used to report Gleason scores from 2-10, but generally today any cancer found with biopsy that is a Gleason 6 is considered low-grade. A Gleason score of 7 is considered medium-grade cancer and Gleason 8 and above is high-grade cancer. The lower the Gleason score, the less likely the cancer is going to spread to the lymph nodes, bones or other organs. Interestingly, if two different patients have a Gleason score 7 cancer, and patient A’s is 3+4=7 and patient B’s is 4+3=7, even though they both have a Gleason score of 7, patient B’s disease is more aggressive because the primary grade was 4. This is an important factor for determining prognosis and influencing treatment options, so it is paramount to accurately determine both your total Gleason score, as well as your primary and secondary Gleason grades.
In a study including 2,500 men with Gleason 6 cancer that had not spread beyond the prostate gland itself, it was observed that cancer recurrence only happened about 1% of the time fifteen years after prostatectomy surgery. Even better news, fifteen years out from surgery the Gleason 6 cancer only spread beyond where it started in the gland less than 0.5% of the time. This has raised the question among researchers: “Is Gleason 6 prostate cancer really cancer or is it something else since it does not metastasize?” Studies continue to help answer this important question.
Magnetic resonance imaging (MRI), when inserted appropriately in the diagnostic work-up of the patient suspected of having prostate cancer, has gained widespread acceptance in the medical community. MRI has adjustable parameters that allow a radiologist to see suspicious areas within the prostate gland that cannot be seen with ultrasound or CAT scan. This makes it possible to perform biopsies under MRI-guidance that target only the area of suspicion rather than randomly sampling areas under ultrasound guidance. Investigators from the Netherlands recently published their findings that trans-rectal ultrasound (TRUS)-guided biopsy underestimates the aggressiveness of prostate cancer (Gleason score) 46% of the time compared to only 5% for MRI-guided biopsy. This is an important consideration for patients when making a choice about how and where to have a prostate biopsy.
As a result of the known morbidity of whole gland therapy for prostate cancer, men are looking for alternatives to whole gland radical treatment. The rate of sexual dysfunction associated with radical prostatectomy is about 50% according to researchers in New York. Urinary incontinence can occur after surgery in 5%-30% of patients. Radiation therapy patients suffer similar side effects. Although the rate of urinary incontinence is less with radiation than surgery, it tends to worsen as the years go by following radiation. Sexual dysfunction rates are about the same as with surgery, but can vary depending on age.
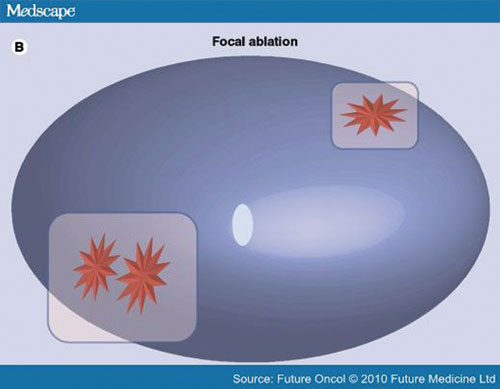
When doctors are caring for patients with low- or medium-grade prostate cancer, they have a lot of choices to make together. Observational strategies include active surveillance and watchful waiting. Active surveillance is the monitoring of a patient and waiting to treat until progression is observed. Watchful waiting is delay of treatment until the patient has symptoms. If the disease progresses to a point where treatment is recommended, it is usually in the form of whole-gland therapy (surgery or radiation) or systemic therapy (hormones to shrink the cancer). What if there was a step in between? Like with breast cancer and cancer of other organs where only the diseased area is treated, doctors and scientists are investigating treating medium-grade prostate cancer with the same philosophy: focal treatment. Energy sources such as heat, cold or various types of non-ionizing radiation (RF, high-intensity focused ultrasound and laser) are being investigated as well as toxic agents applied directly to the prostate cancer, not the entire gland or the entire body. The results for focal therapy of low- or medium-grade prostate cancer are preliminary and investigational, but promising for select men who are unwilling to remain untreated and are unwilling to undergo whole gland therapy.
Dr. Feller is a Board Certified Radiologist at Desert Medical Imaging which has a MRI based prostate cancer program. Please visit their website www.desertmedicalimaging.com for more information or call 760.694.9559.









































Comments (3)
I’ve been diagnosed with prostate cancer. Biopsy was not taken using MRI guidance. Gleason score was 6. I do not know how many of the biopsy tissue showed cancer. The next step is a CT and chest X-ray. Should I be satisfied with their findings, or should I get s second opinion using MRI? And should I have my prostate removed?
Mike – Please see the reply below from Desert Medical Imaging, and thank you for reading Desert Health!
Lauren Del Sarto
Publisher
Prostate cancer diagnosed by random transrectal ultrasound guided biopsy has a published rate of misclassification of about 45%. Talk with your doctor about in-bore MRI targeted biopsy to ensure that you are not harboring a higher grade tumor.
MRI can help delineate the extent of the tumor if nerve sparing surgery is desired and may be helpful for pre-surgical planning.
Once you have an accurate diagnosis of Gleason Score, you can discuss treatment options with your healthcare team.
ALWAYS TALK TO YOUR DOCTOR ABOUT ANY HEALTHCARE DECISION
Learn more about prostate MRI at http://www.desertmedicalimaging.com