The most common disease of the lumbar spine in older people is spinal stenosis, arthritis in the joints of the spine that occurs with aging. The disease has a classic presentation with back pain and aching in the back of the thighs and legs with walking or even standing in the line at the grocery store. Reclining or sitting may relieve it. The neurological examination can be normal. The vascular exam of the lower extremities (LE) is also normal. Yet standing that produces pain in the back and legs is the key symptom that differentiates spinal stenosis from vascular claudication of the LE.
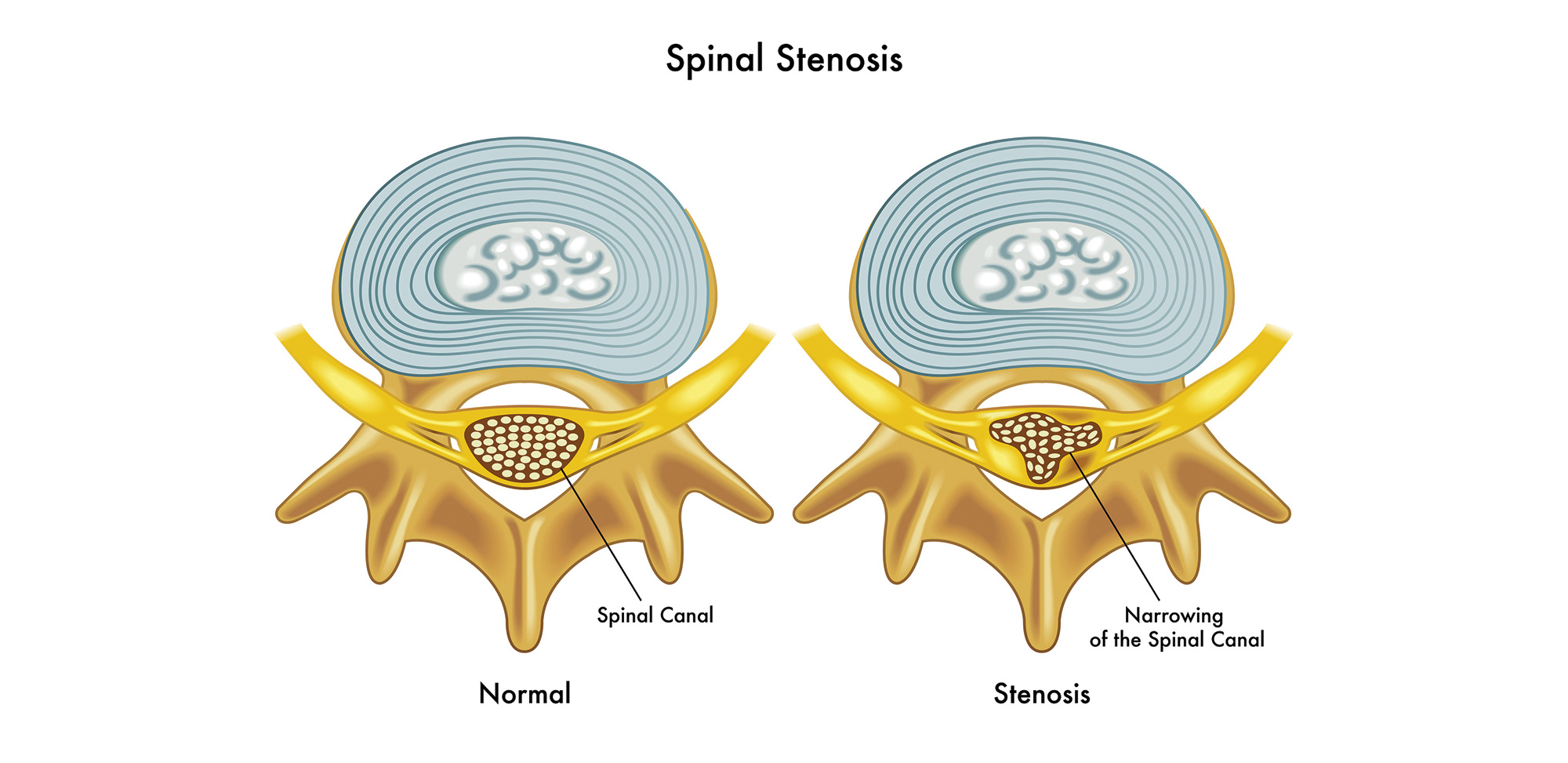
The disease can occur from the forties to the nineties. It is caused by the progressive arthritis at the facet joints of the adjacent lumbar vertebrae. In the normal patient, the facets allow the twisting and bending motions of the spine to maintain its stability. It is these motions that affect these joints, producing arthritic enlargement of the joints with the arthritis, much as it does in the joints of the hand with progressive use. The arthritic joints in the spine can grow in size to be three or four times normal. The bony growth occurs in all directions, but the most damaging is the growth into the spinal canal and into the foramen through which the nerve roots exit the lumbar spine. Thus, the spinal canal narrows, leaving less room for the lumbar roots. This bony pressure places the nerves in the lower spinal canal under pressure, impairing nerve function, and producing weakness of the muscles supplied or pain. Compression of the nerve roots in the spinal canal or foramen will produce a radiculopathy (or pinched nerve) in the LE.
Diagnosis is by a CT, which shows the bony changes in the spine of enlarged facets or ligament hypertrophy, leading to narrowing of the spinal canal. MR imaging shows the nerve roots and their compression.
Treatment can be medical with analgesics initially, not opioids, which can be addictive if used for more than three weeks. Sometimes epidural injections have been helpful. Usually the arthritis progresses as does the symptoms it produces. In those cases surgical decompression can be done. The patient will let you know if they need surgery because their lifestyle becomes compromised. We have operated on patients in their 90s, using special surgical procedures designed to limit the surgery time in the older patient.
Usually after the surgery the patient is in the hospital for a day or two and then is able to walk, in most cases, with much improvement in the pain. Sometimes a fusion is necessary if the adjacent vertebrae are unstable and show slippage of over 4mm in flexion extension films. The results of the surgery are good in a high percentage of cases.
Drs. Etebar and Ausman are part of the Desert Spine and Neurosurgical Institute and members of Desert Doctors. They can be reached at (760) 346.8058 or by visiting www.DesertDoctors.org.












































Comments (0)