Brain metastasis, when cancer cells spread to the brain from primary tumors in other organs in the body, is often regarded with hopelessness. However, new advances in diagnosis and treatment are changing that opinion.
Brain metastasis occurs in up to 50% of patients with cancer. As new systemic treatments prolong life, brain metastases become more common. Quality of life is the most important goal of treatment.
Often a metastasis to the brain is silent and is found on routine screening after the primary cancer is found. Weakness of an arm or leg, speech or visual disturbance, or balance problems are the most common symptoms from larger lesions or smaller metastasis located in critical areas. Headache, nausea and vomiting are non-specific symptoms of increased intracranial pressure. Metastases which produce symptoms are considered for surgical treatment; silent metastases are best considered for stereotactic radiation treatment (SRT).
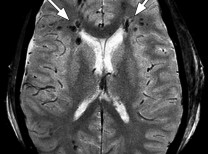
The best imaging modality is contrast-enhanced MR, as CT with contrast can underestimate the number of lesions. Treatment decisions include the following:
- No treatment for those with far advanced disease who have a poor prognosis or whose quality of life cannot be improved.
- Surgery is best for solitary lesions that are accessible. For larger lesions producing symptoms, radiation therapy is not successful. The goal of surgery is to remove the metastasis totally, which will produce the longest survival. Metastasis to the cerebellum will produce rapid death from increased intracranial pressure unless operated, as the cerebrospinal flow is obstructed by the mass and swelling. Radiation often produces more swelling and faster mortality. Removal will provide more time for therapy and even long survivals. In patients with more than one lesion, a combination of surgery and a single treatment of stereotactic radiation therapy (SRT) can be performed to provide quality of life. Surgery can now be done with intraoperative imaging for tumor localization with a high success rate and low morbidity, no mortality, and a short length of stay. Surgery is usually followed with stereotactic focused radiation to the tumor cavity to limit recurrence and prolong survival with quality of life.
- Whole brain radiation therapy (WBRT), formerly relied on as the standard treatment, produces cognitive deficits in patients. SRT can be focused on the lesions and produce lesion regression while preserving cognition and quality of life. SRT can be used in patients with multiple metastases.
- Chemotherapy is used for the primary lesion and for the metastasis. Much more is known today about the molecular factors leading to the seeding and growth of metastases. Recent new molecular treatments can provide remarkable remissions of brain metastasis in patients who previously failed other measures.
- Dexamethazone (4mg every 6hr) is used to reduce the edema associated with brain metastases and can produce rapid symptomatic improvement. Use with proton pump inhibitors. Anti-convulsants are also used prophylactically.
Patients with leptomeningeal carcinomatosis can be treated with a combination of therapies, including shunting for hydrocephalus or reservoir implantation for intrathecal treatment.
All cancers can metastasize to the brain. With the success of modern therapy extending life, brain metastases are becoming more frequent. The most common tumors to metastasize are lung, breast, renal, and colon cancers, and melanoma. Given the many options now available to patients, a discussion by the referring doctor, or the patient with the neurosurgeon, is valuable to be able to review these options.
Dr. Ausman is formerly Head of Neurosurgery at Henry Ford Hospital in Detroit, Michigan and at the University of Illinois at Chicago. He is presently Professor of Neurosurgery at UCLA and Harbor–UCLA Medical Centers and Editor-in-Chief of Surgical Neurology International, a free internet journal of neurosurgery with the largest circulation in the world. He can be reached at Desert Spine and Neurosurgical Institute (760) 346.8058 or at jamesausman@mac.com. He is also a member of Desert Doctors. DesertDoctors.org or call (760) 232.4646.














































Comments (0)