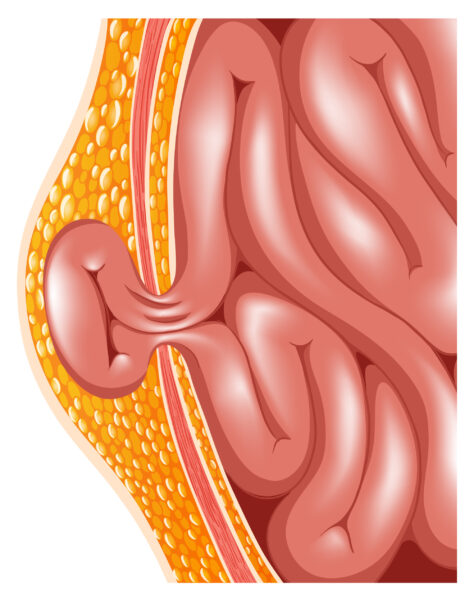
The easiest way to think about a hernia is as a hole in your abdominal wall. Whether at your groin, belly button or an old incision, a hernia is a hole. This allows intra-abdominal contents to protrude through the hole creating a bulge which may be accompanied by pain or discomfort. Hernias tend to be reducible meaning that when you press on them or lay down, the contents “reduce” back into the abdomen. They can become incarcerated where the contents do not reduce no matter what the patient does. Worse cases may experience strangulation, where the herniated contents lose blood supply. It is important to know that an incarcerated hernia may be a surgical emergency to avoid strangulation.
Traditional open repair surgery attacks a groin hernia from the top with an incision in the lower abdomen. The vast majority of open hernia surgeries are done by placing a mesh sheet to cover or patch the hole. With advances in minimally invasive laparoscopic surgery, the mesh patch can be placed on the underside of the hole with much smaller incisions. Robotic surgery takes this one step further by improving the view through the camera and increasing the precision with which the surgery is done.
Patients tend to get wide-eyed when a surgeon suggests a robotic approach. They have visions of the surgeon unleashing a robot and going to have a cup of coffee while the robot completes the surgery. Robotics is more like remote control surgery. The surgeon sits down at a console after setting up the robot. His or her hand motions are then translated to the motions of the instruments inside the patient. It is truly like having your hands inside the patient through tiny holes. Following are the most important advantages of robotic surgery over traditional laparoscopic surgery for groin hernias:
Decreased postoperative pain. I see far more patients return for their postoperative visit with minimal to no pain compared with open or laparoscopic procedures. This reduces the need for narcotic pain medication.
Ability to repair hernias on both sides. Through the same three small incisions, hernias on both sides can be fixed at the same time. Gone are the days of needing to choose which side to fix first and 3 to 6 months later have the other side fixed. About 20 percent of the time, when a patient presents with a hernia on a single side, one is discovered on the other side.
Total control. With traditional laparoscopic surgery, a surgeon can use only his or her two arms. They must rely on an assistant for any additional instruments and the camera. With robotics, the surgeon can control up to four arms by continually switching back and forth as necessary. When the surgeon positions the camera, the robot does not move or shake until the surgeon repositions.
It is important to discuss options for hernia repair techniques with your surgeon and to choose a modality with which both of you are comfortable.
Dr. Reckard is a general surgeon and chair of the Department of Surgery at Eisenhower Health. He is also a member of Desert Doctors and can be reached at (760) 776.7600. www.DesertDoctors.org













































Comments (0)