In 2015 more people in the United States died from drug overdose than car accidents and gun homicides combined.1 It is no secret that our country is going through an opioid epidemic. How did we get here? And if not with medication, then how should we be treating pain?
Studies in the 1980s indicated little concern about the risks of prescribing opioids for pain and pharmaceutical companies began heavily marketing drugs such as oxycodone, hydrocodone, and codeine. Current reports from the CDC indicate that 91 people die from opioids in the United States every day. A researcher from the University of Arkansas found that if a person is prescribed a ten-day course, there is a 20 percent chance they will still be on pain killers one year later. In addition to their highly addictive nature, opioids are often a poor choice for pain. In recent studies these drugs were shown to lack effectiveness with treating chronic low back pain.2 Why would they be effective? Their purpose is to reduce the sensation of pain by interrupting the signal of pain to the brain.
It is time we start treating the cause of symptoms and not the symptoms themselves.
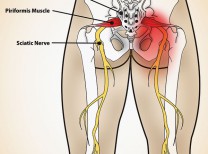
Musculoskeletal pain such as low back, neck, and knee pain and osteoarthritis account for a large portion of the visits to health care professionals. Pain is a complex symphony of a stress, or perceived stress, on the body which sends a signal through the nervous system to the brain, where it is interpreted and distinguished as a threat or not. If the brain determines it to be a problem, we experience the sensation of pain. As previously noted, opioids simply reduce the sensation of pain by interrupting the signal to the brain. The stress that started the warning system is never addressed. Many times that stress on our knees, neck, shoulders or low back can be caused by incorrect habitual movement, weakness, poor muscle control, or lack of mobility. Addressing these issues through prescribed exercise is a much more effective way to treat the problem. The Centers for Disease Control (CDC) notes evidence that exercise as part of physical therapy intervention is effective in treating low back pain, hip pain, knee osteoarthritis and fibromyalgia.3
Our outlook on pain management is promising. The current guidelines from the American College of Physicians (ACP) for treating low back pain are consistent with the CDC recommendations. The group recommends spinal mobilization for acute low back pain.4 Spinal mobilizations are performed by physical therapists, doctors of osteopath and chiropractors. A study in Spine supports the findings, stating that patients have a 95 percent chance of a favorable outcome with spinal manipulation if certain criteria are present5; one of the criteria is the presence of pain for less than 16 days. For chronic low back pain lasting longer than 90 days, the ACP recommends exercise and other components of physical therapy as well.
For far too long we have been treating the symptoms and not the cause of pain. The evidence and shift in health care towards treating musculoskeletal pain with exercise and movement is promising. In addition to better outcomes, these interventions are much safer than the use of opioids.
Vincent Kambe, PT, DPT, OCS is the clinic director for Avid Physical Therapy. He is a doctor of physical therapy and orthopedic certified specialist and can be reached at vince@avidphysicaltherapy.com
References: 1) Center for Disease Control and Prevention. National Center for Health Statistics; 2) Steffens D., Mahen C., et. Al. Prevention of Low Back Pain: A Systemic Review and Meta-Analysis. Jama Intern Med. 2016 Feb, 176(2) 199-208; 3) Dowell, D., Haegerich, T., Chou, R. CDC Guidelines for Prescribing Opioids for Chronic Pain. Recommendations and Reports. 2016 March, 65(1); 1-49; 4) Qaseem A., Wilt T., McLean R. Noninvasive Treatment for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline from the American College of Physicians. Annals of Internal Med. 2017 April, 166(7); 514-530; 5) Flynn T., Fritz J., Whitman J. et Al. A clinical Prediction Rule for Classifying Patients with Low Back Pain who Demonstrate Short-Term Improvement with Spinal Manipulation. Spin. 2002 December, 27 (24); 2835-2843.








































Comments (0)